Progression of Atherosclerosis and Plaque Vulnerability in ASCVD
Atherosclerotic plaques represent the hallmark lesion of atherosclerosis. While some plaques remain asymptomatic, some become obstructive causing stable angina, and others can become vulnerable to rupture and acute thrombosis which may lead to an acute coronary syndrome.1,2
Interactive Artery
Check out this interactive artery showing the progression of atherosclerosis and vulnerable plaque.


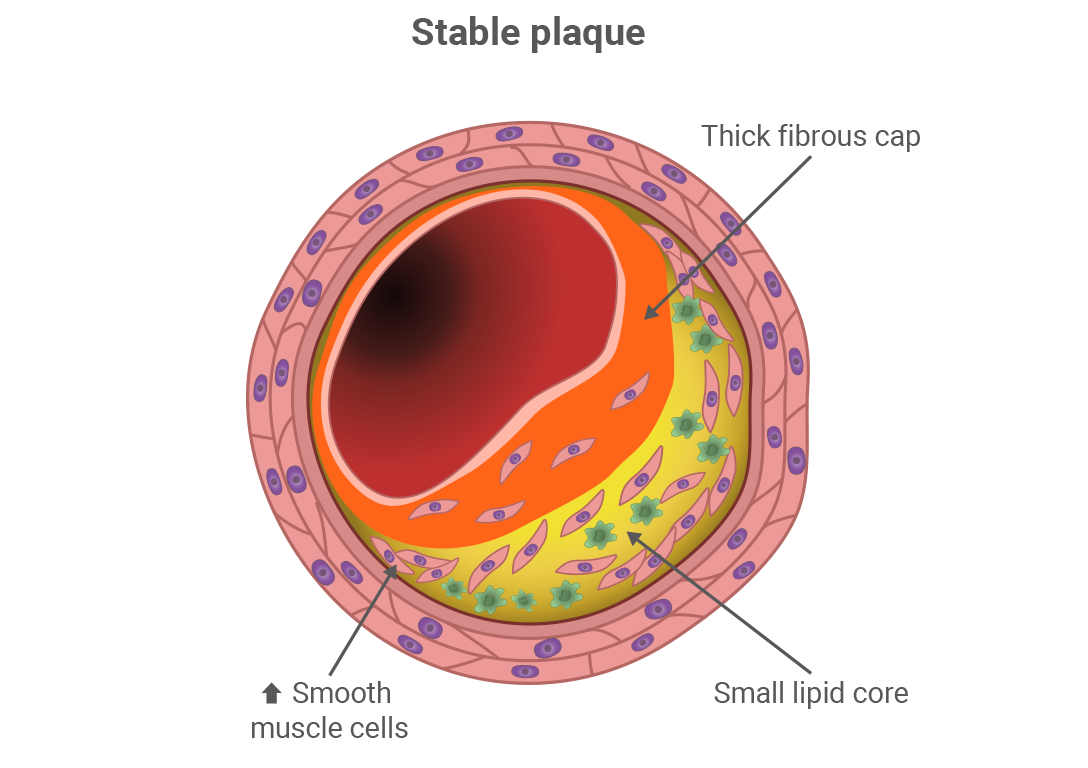
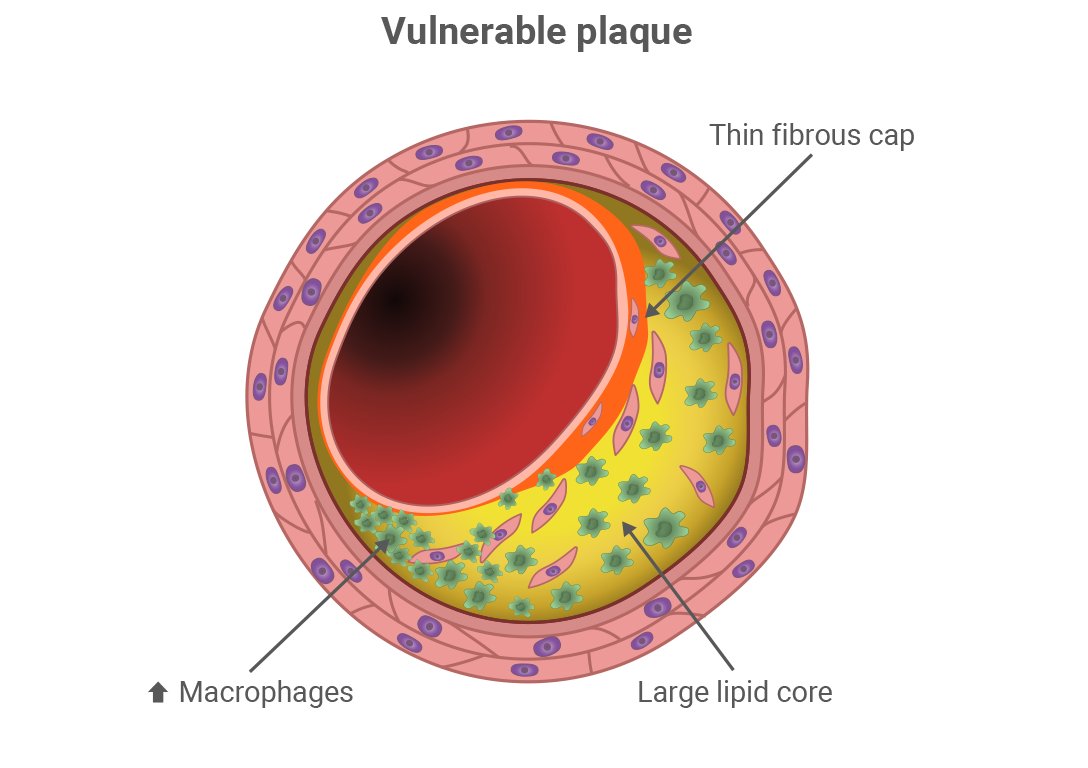
Coronary Plaque Composition and Vulnerability
- Vulnerable plaques are characterized by a thin fibrous cap (< 65 μm), a large lipid-rich or necrotic core (lipid arc> 90 degrees), and presence of inflammatory cells2-5
- Grundy SM, Arai H, Barter P, et al. An International Atherosclerosis Society Position Paper: global recommendations for the management of dyslipidemia – full report. J Clin Lipidol. 2014;8(1):29-60. doi:10.1016/j.jacl.2013.12.005.
- Stefanadis C, Antoniou C-K, Tsiachris D, Pietri P. Coronary atherosclerotic vulnerable plaque: current perspectives. J Am Heart Assoc. 2017;6(3):e005543. doi:10.1161/JAHA.117.005543.
- Singh RB, Mengi SA, Xu Y-J, Arneja AS, Dhalla NS. Pathogenesis of atherosclerosis: a multifactorial process. Exp Clin Cardiol. 2002;7(1):40-53.
- Bentzon JF, Otsuka F, Virmani R, Falk E. Mechanisms of plaque formation and rupture. Circ Res. 2014;114(12):1852-1866. doi:10.1161/ CIRCRESAHA.114.302721.
- Mushenkova NV, Summerhill VI, Zhang D, Romanenko EB, Grechko AV, Orekhov AN. Current advances in the diagnostic imaging of atherosclerosis: insights into the pathophysiology of vulnerable plaque. Int J Mol Sci. 2020;21(8):2992. doi:10.3390/ijms21082992
Effect of LDL-C Lowering on Atherosclerotic Plaque
Impact on Vulnerable Plaque
Statin trials using optical coherence tomography (OCT), a catheter-based coronary artery visualization technique, demonstrate that achievement of lower LDL-C levels with more intensive therapy is associated with increased fibrous cap thickness (FCT) and smaller lipid arc, thus favorably improving features of vulnerable plaque.1-3
LDL-C Lowering Has Been Shown to Improve Key Features of Vulnerable Plaque1
Achieving lower LDL-C levels was shown to be associated with smaller lipid arc and thicker fibrous cap1




Patients in the study were stratified according to achieved LDL-C levels (< 50 [87 plaques], 50–70 [81 plaques], 70–100 [117 plaques], < 100 mg/dL [130 plaques]). Data analyzed from the Cleveland Clinic FD-OCT Registry, which included 293 and 122 non-obstructive lipid and fibrous plaques in 280 stable statin-treated CAD patients evaluated by FD-OCT imaging in vessels requiring PCI.
CAD, coronary artery disease; FD-OCT, frequency-domain optical coherence tomography; LDL-C, low-density lipoprotein cholesterol; PCI, percutaneous coronary intervention.
Impact on Atherosclerotic Burden
Numerous clinical trials using another imaging technique, Intravascular Ultrasound (IVUS), have assessed the impact of LDL-C lowering on atherosclerotic burden. These studies have demonstrated a direct relationship between LDL-C lowering and reduction in atheroma volume.1-5
LDL-C Lowering Has Been Shown to Decrease Atherosclerotic Burden4

*SATURN: Effects of High-intensity Statin vs. High-Intensity Statin; †REVERSAL: Effects of High-intensity Statin vs. Moderate-intensity Statin; ‡ILLUSTRATE: Effects of Statin + CETP inhibitor vs. Statin + Placebo
CETP, cholesteryl ester transfer protein; LDL-C, low-density lipoprotein cholesterol; PAV, percent atheroma volume.
- Kataoka Y, Hammadah M, Puri R, et al. Plaque microstructures in patients with coronary artery disease who achieved very low low-density lipoprotein cholesterol levels. Atherosclerosis. 2015;242(2):490-495. doi:10.1016/j.atherosclerosis.2015.08.005.
- Tardif J-C, Lesage F, Romeo P, Pressacco J. Imaging biomarkers in atherosclerosis trials. Circ Cardiovasc Imaging. 2011;4(3):319-333. doi:10.1161/circimaging.110.962001.
- Mushenkova NV, Summerhill VI, Zhang D, Romanenko EB, Grechko AV, Orekhov AN. Current advances in the diagnostic imaging of atherosclerosis: insights into the pathophysiology of vulnerable plaque. Int J Mol Sci. 2020;21(8):2992. doi:10.3390/ijms21082992.
- Puri R, Nissen SE, Ballantyne CM, et al. Factors underlying regression of coronary atheroma with potent statin therapy. Eur Heart J. 2013;34(24):1818-1825. doi:10.1093/eurheartj/eht084.
- Daida H, Dohi T, Fukushima Y, et al. The goal of achieving atherosclerostic plaque regression with lipid-lowering therapy: Insights from IVUS trials. J Atheroscler Thromb. 2019;26:592-600. doi.org/10.5551/jat.48603.
Plaque Imaging Modalities
Different intravascular techniques including optical coherence tomography (OCT) and intravascular ultrasound (IVUS) can be used to visualize atherosclerotic plaques. Each technique offers complementary information about plaque, with IVUS providing insight into plaque volume, and OCT allowing for detection of certain features of plaque vulnerability.1-3
IVUS Measures the Extent and Distribution of Atherosclerotic Plaque, Allowing Assessment of Changes in Plaque Burden2,3
Intravascular ultrasound (IVUS) produces cross-sectional images of the lumen and coronary artery wall using catheter-based ultrasound transducers, reaching 100 μm resolution. Due to deeper tissue penetration, IVUS enables volumetric quantification of atheroma (plaque size) within the entire vessel wall from intima to adventitia, and allows for evaluation of changes in plaque burden over time.
OCT Offers High Resolution Necessary to Detect Characteristics of Vulnerable Plaque Including Lipid Core and Fibrous Cap2,3
Optical Coherence Tomography (OCT) produces cross-sectional images of the lumen and the superficial (intimal) layer of the arterial wall by measuring near-infrared light intensity reflected from tissue. OCT provides the highest spatial resolution capability (<10μm), allowing for higher sensitivity to detect certain features of plaque vulnerability, including the fibrous cap and the lipid core.
Comparison of OCT and IVUS Imaging Modalities to Assess Plaque Characteristics2,3


CS, clinical studies; CA, clinically approved for commercial use
- Dweck MR, Doris MK, Motwani M, et al. Imaging of coronary atherosclerosis – evolution towards new treatment strategies. Nat Rev Cardiol. 2016;13(9):533-548. doi:10.1038/nrcardio.2016.79.
- Tardif JC, Lessage F, Harel F, Romeo P, Pressacco J. Imaging biomarkers in atherosclerosis trials. Circ Cardiovasc Imaging. 2011;4(3):319-333. doi:10.1161/CIRCIMAGING.110.962001.
- MacNeill BD, Lowe HC, Takano M, Fuster V, Jang IK. Intravascular modalities for detection of vulnerable plaque: current status. Arterioscler Thromb Vasc Biol . 2003;23(8):1333-1342. doi:10.1161/01.ATV.0000080948.08888.BF